









Latest Post

MEDICAL WASTE INCINERATOR (50 C 60kg/hr)

Support Health Sector Support Project
Point of Installation (Hospitals) Moi Voi, Makindu, Maragua, Eldama Ravine and Isiolo District Hospitals
1. General Description
Supply, delivery, installation and commissioning of a medical waste incinerator suitable for disposal of Medical, General and Pathological waste in a safe and clean environment. The unit shall consist of two chambers and operate on the principal of controlled air and temperature. The unit shall consist a particulate remover (scrubbers) as stipulated in waste management regulations, 2006 (Legal notice NO. 121 of 29th September, 2006). The Unit shall be fully automatic and controlled by an automatic electronic controlled system except loading system which shall be manual. The unit shall be capable of incinerating between 50 to 60 kg of solid medical waste per hour. It shall be constructed from mild or aluminized steel lined with refractory material.
Main unit
Application For incineration, general and pathological
Capacity 50 C 60 kg/h burn rate
Type Two combustion chambers type; primary and Secondary, controlled/forced combustion air type with a flue gas emission scrubbing unit
Operating time Minimum 8 hours daily
Operating temperature From 850 0C to 1200 0C, Automatic controlled
Residual Ash 5 to 10%
3.2 Primary Chamber
Construction Constructed from heavy duty mild or aluminized steel Or
equal and approved equivalent
Insulation material Refractory material lining similar or equal to calcium
Silicate and hot face combination of heavy duty brickwork
Internal Construction Fixed hearth type complete with gratings, concave bottom
and charging door, lined with refractory material
Charging Door Suitable for manual loading of wastes and with smooth
Dear seal equivalent of Ceramic seals with hinges.
Door Lock Automatic, Electric type
Ash removal door Provided, for removing resultant bottom ash leftovers from the Primary chamber
Gratings Provided
Loading Manual loading of waste
Primary Burner Fully automatic, with fuel, temperature and speed controls with ignition system, flame detector, Air fan complete with safety features, flame failure, Diesel fired fuel injector type and Flange mounted
Blower Provided. For supplying excess combustion air through the distribution system with speed control system
Temperature Minimum exit 850 0C
Observation port To be provided with protective glass type
Construction Constructed from heavy duty mild or aluminized steel or equal and approved equivalent
Insulation Refractory material lining
Combustion Temperatures Above 850 0C, controlled electronically
Gas residue or retention Time > 2 second at minimum 850 0C
Secondary Burner Provided, Diesel fired, fully automatic, with fuel, temperature and speed controls, With ignition system, Flame detector, Air fan, Complete with safety features, flame failure Diesel fired fuel injector type. Flange mounted
Ejector Provided, Venturi type, for cooling the flue gases
Combustion Air Fan Provided for supplying combustion and creating a negative drift and turbulences
Temperature Maximum 1600 0C
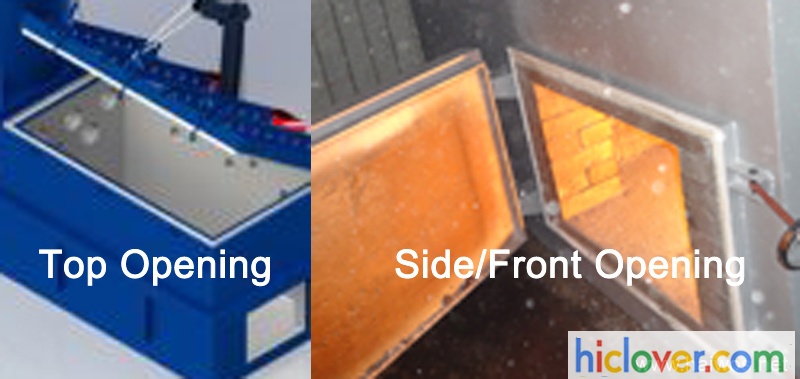
Waste Incinerator Door: Side/Front Opening Door VS. Top Opening Door
|
Things |
Side Loading Door |
Top Loading Door |
|
Suggestion |
|
|
|
Cost |
Affordable |
High expense |
|
Manufacture Tech. |
Easy |
A clutter tough |
|
Safty |
safe |
a lot more protected |
|
Burner Creating |
L/ I |
L |
|
Filling up |
hands-on |
huge door can be by Forklift |
|
Land job |
little |
big |
|
Ash door |
exact same with feeding door or alone |
alone |
|
market share |
Most-CHINA/USA/INDIA |
Couple Of- UK/USA |
|
Dooring open type |
Hands-on |
Pry bar/Hydraulic stress and anxiety |
|
Dooring Open up measurement |
little |
huge |
|
Better for |
clinical bag waste |
pet waste |
|
open when shedding |
safer, can feed waste, couple of smoke |
not secure, can not feed waste, most smoke |
Tel: +86-25-8461 0201
Website: www.hiclover.com
Email: [email protected]
Email: [email protected]


Ebola: livestock incinerator imported from Europe to cremate corpses
Ebola: livestock incinerator imported from Europe to cremate corpses
‘I have never seen this number of bodies before’: Life at an Ebola clinic in Liberia
Scale of Ebola outbreak in Western Africa leaves staff of frontline health agency with grim decisions over who to treat and who to turn away.
Like every other volunteer who serves with Médecins Sans Frontières, Stefan Liljegren joined up to help the sick and destitute. In 15 years with the agency, he has been everywhere from Afghanistan and Kosovo through to South Sudan and East Timor, the hard and often dangerous work compensated for by the knowledge that he is saving lives.
His latest mission, in Ebola-hit Liberia, offers rather less job satisfaction. As field co-ordinator of MSF’s new 160-bed Ebola treatment centre in the capital, Monrovia, one of his tasks is to decide which of the sick people who arrive outside the clinic’s gates should get treatment. Such is the scale of the outbreak that for every 20-30 new patients the clinic admits each day, the same number are often turned away – despite the likelihood that they will go home and infect their relatives
“This is by far the most difficult challenge that I have ever faced,” the 44-year-old Swede told The Telegraph during a brief break from his work in the sweltering humidity of Liberia’s monsoon season. “Every day I have been faced with impossible choices, and decisions that are inhuman to make. Having to tell someone that they can’t come in when they are screaming and begging to do so is an indescribable feeling, especially when you know they may go back to families who might well then get sick themselves.”
Outside the clinic an hour earlier, a grisly scene demonstrated Mr Liljegren’s point. Resting face down in the mud was the body of Dauda Konneh, 42. He had been lying there dead since daybreak.
“He was vomiting a lot and had symptoms like Ebola, so we put him in a pick-up truck and took him here for treatment,” said one young man outside. “When we got here last night, he was still alive, but the clinic would not accept him. He died at dawn today.”
When The Telegraph mentions this to Mr Liljegren, he nods. Having dead or dying patients outside the clinic overnight is “a regular occurrence,” he says. The reason being that once night falls, the hospital does not admit anyone: handling Ebola patients requires extreme care at the best of times, and it would be dangerous to do so in the dark.
The task of removing Mr Konneh’s body falls to Stephen Rowden, a British MSF volunteer from Danbury, Essex, who leads a team in charge of the safe removal of corpses, which are sprayed with chlorine-based disinfectant first. “When I started it was maybe a body every two days, now it is daily and sometimes up to five a day,” said Mr Rowden, 55. “I have never seen this amount of bodies before. It sounds callous, but you just have to switch off emotionally.”
No amount of “switching off”, though, spares the MSF staff from the wider scale of the fatalities around them. The clinic, one of three now operating in Monrovia, has seen 350 deaths in the last month alone. Since all infected bodies have to be burned, the casualties have exceeded the ability of Monrovia’s local crematorium to cope. MSF has had to import an incinerator from Europe – normally used for livestock – to assist. For an aid agency that prides itself on triumphing in even the most difficult operating circumstances, it is a depressing reminder of how far there is to go.
The challenges facing the MSF clinic are in turn a snapshot of the wider outbreak now engulfing West Africa. On Tuesday, a World Health Organisation study warned that the number of Ebola cases – currently topping 5,000 – could reach hundreds of thousands by January unless the aid operation was drastically increased.
Nowhere is the problem more acute than in Liberia, where 40 per cent of all the deaths have taken place, and where the government health service – already badly damaged by the 1989-2003 civil war – has been paralysed by Ebola infections among its own staff. In coming weeks, a 3,000-strong US military mission will arrive in Monrovia to build 17 more Ebola treatment clinics. But MSF, which worked in Liberia throughout the civil war, says the situation is already spiraling out of control.
Inside the MSF clinic in Monrovia, those patients fortunate enough to get through the gates are admitted to rows of large white treatment tents. The clinic is designed so that only staff clad in the yellow high protective gear can enter the “high risk” wards, where those with advanced stages of the virus are treated.
In the nurses’ area, meanwhile, a pair of paperwork folders hung next to the door describe the patients’ only possible outcomes. One has a set of forms marked “Discharge”, given to the few who manage to fight the virus off. The other has a set of forms marked “Death Certificate”. Right now, the latter is used between 70 and 80 per cent of the time.
In another section, patients who have tested positive but are not yet acutely ill congregate in an open air living room, where they can chat to each other, do exercises, and play board games.
One patient, Foofee Sheriff, 54, tells how he became infected after attending the funeral of his brother, who died recently. “We did not touch my brother’s body during the burial, we used plastic bags on our hands to make sure that didn’t happen,” he insists. “But eight days after I started feeling sick.”
Mr Sheriff’s claim not to know how he became infected is typical. It may be that he genuinely does not know. Or it may be that he failed to take adequate precautions at his brother’s funeral but does not wish to admit it.
Either way, it makes it all the harder for the medical staff to establish patients’ so-called “contract traces”, which, in an ideal world, identify exactly who else might have been infected. This would also be useful in the case of Mr Konneh, who, according to the man who brought him in, worked for Irish aid agency Concern, which itself has been conducting a public health campaign about how to avoid getting Ebola.
Alerted by The Telegraph the following day, Concern confirmed that Mr Konneh, a father-of-two, did indeed work for them, although they believe he may have died from an existing medical condition which took a turn for the worse in the past ten days. Such is Ebola’s grip on Liberia, however, that right now, any sudden illness is feared to be the virus – hence Mr Konneh’s attempt to reach the clinic. The young man adds that Mr Konneh moved between two different households while sick, and that the occupants of both houses are “now very worried”.
As too is Mr Liljegren, for whom there is simply no telling how many more desperate people may soon be pleading outside his clinic’s gates. “It gets worse by the day,” he says. “How much worse it will it get? I have no idea.”
http://www.telegraph.co.uk/news/worldnews/ebola/11118025/I-have-never-seen-this-number-of-bodies-before-Life-at-an-Ebola-clinic-in-Liberia.html

Industrial Incinerator
Basic Info.
Additional Info.
Product Description
Key Features: * All models with Dual combustion chamber. * Stainless Steel chimney/stack, long life. *according to order * High fever, long life of incinerator. * Free or minimum installation on site. * High speed, from 10kgs to 500kgs per hour, up to 6ton daily. *according to order * New Design for pet animal cremation enterprise. * One year guarantee on incinerator and parts in stock. Nanjing Clover Medical Technology Co., Ltd.. Is a leading waste incinerator manufacturer in China. We’re local producer and one of the largest exporter of China. Pyrolytic incinerator gear technical is main waste treatment all of the world, for Medical Waste, Animal Incineration, Pet cremation and other good wste. The capacity from 10kgs/Hr. To 500kgs/Hr. , up to 6ton daily. Presentlywe provide different series for local client requirements and united states monster incinerators available, us crematorium manufacturer, usa medical waste incinerator, use natural gas incinerator, used batch load creature incinerators for sale by owner, layout updated incinerator with our leading technology. The updated design characteristic of our range of incinerators create them one of the most cost effective in the world.
| Items/Model | TS10(PLC) | TS20(PLC) | TS30(PLC) | TS50(PLC) | TS100(PLC) |
| Burn Rate | 10 kg/hour | 20 kg/hour | 30 kg/hour | 50 kg/hour | 100 kg/hour |
| Feed Capacity | 20kg | 40kg | 60kg | 100kg | 200 kg |
| Control Mode | PLC | PLC | PLC | PLC | PLC |
| Combustion Chamber | 100L | 210L | 330L | 560L | 1200L |
| Internal Dimensions | 50x50x40cm | 65x65x50cm | 75x75x60cm | 100x80x70cm | 120x100x100cm |
| Secondary Chamber | 50L | 110L | 180L | 280L | 600L |
| Smoke Filter Chamber | Yes | Yes | Yes | Yes | Yes |
| Feed Mode | Manual | Manual | Manual | Manual | Manual |
| Voltage | 220V | 220V | 220V | 220V | 220V |
| Power | 0.5Kw | 0.5Kw | 0.5Kw | 0.7Kw | 0.7Kw |
| Oil Consumption (kg/hour) | 5.4–12.6 | 7.8–16.3 | 10.2–20 | 12.1–24 | 14–28 |
| Gas Consumption (m3/hour) | 6.2–11.4 | 8–15.7 | 9.8–20 | 9.9–26.1 | 10–32.2 |
| Temperature Monitor | Yes | Yes | Yes | Yes | Yes |
| Temperature Protection | Yes | Yes | Yes | Yes | Yes |
| Oil Tank | 100L | 100L | 100L | 100L | 200L |
| Feed Door | 30x30cm | 45x40cm | 55x50cm | 70x55cm | 80x60cm |
| Chimney | 3Meter | 3Meter | 5Meter | 5Meter | 10Meter |
| Chimney Type | Stainless Steel | Stainless Steel | Stainless Steel | Stainless Steel | Stainless Steel |
| Residency Time | 2.0 Sec. | 2.0 Sec. | 2.0 Sec. | 2.0 Sec. | 2.0 Sec. |
| Gross Weight | 1500kg | 2200kg | 3000kg | 4500kg | 6000kg |
| External Dimensions | 140x90x120cm | 160x110x130cm | 175x120x140cm | 230x130x155cm | 260x150x180cm |

Waste Incinerators
Basic Info.
Additional Info.
Product Description
First, we are one maker in China. We are in this field from year 2005 and in the time, we create trading company to oversea. Under assistance of our client, such as our agent in Egypt, Mr. Ibrahim, solid waste incinerator boiler producers, solid waste incinerator gas, solid waste incinerator korea, solid waste incinerator brand new hampshire, we start to expand our incinerator enterprise. We have our own workshop in Nanjing town liuhe economical zone and we have 20-30 employees. Up to now, oversea market is own main market and from year 2011, we’ll dig China market.